Benjamin Mateus
It is a known national embarrassment that among OECD countries, the United States ranks 30th in its maternal mortality death rates, only behind Mexico.
In 2000, the Millennium Summit of the United Nations established eight international development goals for the year 2015 that were adopted by the 191 member states. One of these goals was to decrease the maternal mortality rates globally by 75 percent.
A Lancet 2016 systematic analysis of this global effort highlighted that only 10 countries achieved the reduction in maternal mortality rate (MMR) of 75 percent in the period from 1990 to 2015. Overall, global maternal deaths did decline by 30 percent. Most of those reductions occurred after the Millennium declaration.
However, the MMR increased in 26 countries, including a 56 percent rise in the US from 16.9 deaths per 100,000 in 1990 to 24.7 deaths in 2015. Luxembourg, Canada and Greece were the other developed countries with a rise in MMR, but their overall rate is still two to three times lower by comparison. The other countries with rising MMR include many of the sub-Saharan African nations as well as islands such as Jamaica, Saint Lucia, American Samoa and Guam.
The World Health Organization (WHO) defines maternal death as the death of a woman while pregnant or within 42 days of termination of the pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.
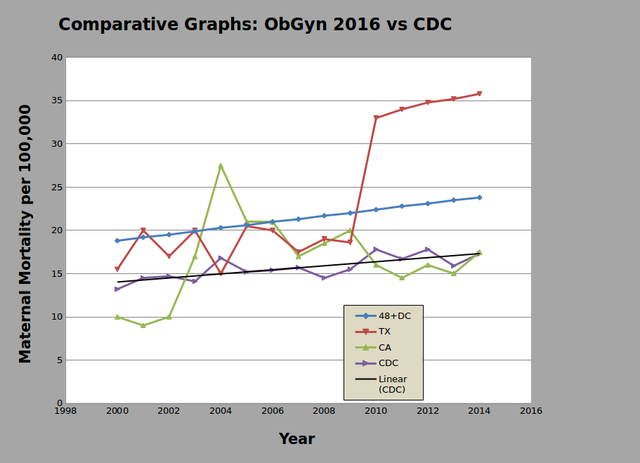 Maternal mortality rates for 48 US states, Washington DC, Texas and California, from data published by The American College of Obstetricians and Gynecologists, and MMR from the CDC.
Maternal mortality rates for 48 US states, Washington DC, Texas and California, from data published by The American College of Obstetricians and Gynecologists, and MMR from the CDC.
In 2000, the US Department of Health and Human Services (HHS) set a national goal for maternal death no higher than 3.3 deaths per 100,000 live births by 2010. In that year, the Centers for Disease Control and Prevention (CDC) reported an MMR rate of 13.2. Despite this national goal, the CDC reported that the US MMR had risen to 17.8 by 2009. Yet, many had argued that these reported statistics were still well below the actual magnitude. Delays in adopting the new standards for reporting maternal deaths, using nonstandard questions or having no pregnancy questions on the death certificate, made them unreliably low.
Maternal death rates are calculated by collecting the data from death certificates. These are compiled by each state and reported to the CDC’s Pregnancy Mortality Surveillance system. In the US, the manner in which death certificates were filled out and their relation to pregnancy were inconsistent and did not capture the relationship of that death to a woman’s pregnancy.
Before 2003, only three states collected data according to the WHO criteria. Fifteen states had pregnancy questions with variable timeframes from termination of pregnancy to the death, while 32 states and Washington DC did not have pregnancy questions on their death certificates.
It was only in 2003 that the HHS secretary approved revisions to the death certificate that captured pregnancy related questions. However, only four states—New York, Montana, Idaho and California—adopted these changes immediately. California elected to capture a one-year period on their death certificate versus 42 days, thereby combining both maternal and late maternal deaths. It would take another 11 years for 44 states and Washington DC to trickle in and implement these changes. Virginia was the last state to adopt the revision to the death certificate in 2017.
A damning study was published in 2016 in Obstetrics and Gynecology, titled “Recent Increases in the US Maternal Mortality Rate: Disentangling Trends from Measurement Issues.” The observational study “analyzed vital statistics from maternal mortality data from all US states in relation to the format and year of adoption of the pregnancy question [on their state death certificate].” The CDC’s National Center for Health Statistics is the official source for the reporting of MMR in the US and comparison with other nations as reviewed above. Studies conducted before 2003 had noted an under-reporting of maternal deaths in the National Vital Statistics System and are considered inaccurate. This study intended to address this discrepancy.
As the authors note, maternal deaths are rare events and therefore difficult to analyze state by state, except in the most populous. Reportedly there were 396 deaths in 2000, increasing to 856 deaths in 2014. They examined California separately because it chose to define maternal mortality within one year of pregnancy instead of 42 days per the WHO guidelines. Though Texas adopted revisions to their death certificate in 2006, they were analyzed separately because of a sharp rise in 2010 that saw maternal mortality double. The data for the other states and Washington DC were combined into four groups, according to when they initiated revisions to their death certificates.
“Unadjusted data from all states regardless of revised death certificates demonstrated that US maternal mortality more than doubled from 9.8 deaths per 100,000 in 2000 to 21.5 in 2014,” the study notes.
For group 1 (24 states and Washington DC) who did not have a pregnancy question on their death certificate in 2003, but had made revisions to their death certificates before 2013, the statistical modeling adjusted mortality rate provided a correction factor of 1.932. That means they adjusted for the undercounting in the years before revision such that the new MMR was calculated at 18.2 in 2000, increasing to 22.8 in 2014.
For group 2 (14 states) that had a nonstandard pregnancy question, the correction factor was 2.067, changing the MMR to 18.4 in 2000 and rising to 24.5 in 2014.
Group 3 included eight states that had not revised their death certificates as of late 2013 and could not be adjusted for their analysis. Not surprisingly their rates are lower, at 8.0 to 10.4 in the intervening years. Group 4 comprised three states that followed the WHO guidelines. Their MMR was 14.0 in 2000, rising to 19.9 by 2014.
Though Texas revised its death certificate in 2006, it was analyzed separately. Adjusted MMR for 2000 to 2010 was 17.7 to 18.6. After 2010, a sharp twofold rise was seen, jumping to 33.0 in 2011 and rising to 35.8 by 2014. The authors note that this data remains puzzling and unexplained. They write, “In the absence of war, natural disaster, or severe economic upheaval, the doubling of a mortality rate within a 2-year period in a state with almost 400,000 annual births seems unlikely.”
When California adopted revisions to their death certificate, their MMR doubled from 10 in 2003 to 21.5 to 2004. The state moved to implement measures that addressed postpartum hemorrhage and hypertensive disorders that contributed to the reduction in mortality as seen in the graph.
Maternal deaths revised upward
Overall, the study found that adjusted MMR for 48 states and DC was 18.8 in 2000 and rose to 23.8 by 2014, an increase of 26.6 percent. This data was based on 7,269 maternal deaths and 46,722,133 live births in the intervening years. Twenty percent of the observed increase in the unadjusted rise was the result of a real increase in maternal mortality, and 79.9 percent was the result of improved ascertainment.
It is a scandal that the richest country in the world has a chronic underfunding of the state and national vital statistics system such that accurate and reliable data cannot be obtained to enact necessary timely changes. By any standard in the financial sectors, an 80 percent disparity in such accounting would have the news media clamoring to report the event and congressional hearings would follow in days, with senators demanding answers to such negligence. But this is intentional if viewed from a socioeconomic perspective. If this were considered important, then resources would be directed to nationalizing and augmenting the woefully lacking maternal services in the US.
Four million women give birth each year in the US. Pregnancy remains the top reason for admission to the hospital. Where such statistics could garner attention and demand action, for nearly 15 years we have remained blind to this existing travesty. The US has no national review of maternal deaths.
Given the projected shortage of 8,000 to 9,000 physicians and midwives by 2023, the impending cuts to Medicare, and virtually zero interest within the two big business parties to address the crisis of maternal health care, there is little chance to correct this without a concerted effort on the part of the working class to demand accountability as part of the overall fight to replace the for-profit health care system with socialized medicine.
No comments:
Post a Comment