Gail E. Tverberg
We would like to think that we can eliminate COVID-19, but doing so is far from certain. The medical system has not been successful in eliminating HIV/AIDS or influenza; the situation with COVID-19 may be similar.
We are discovering that people with COVID-19 are extremely hard to identify because a significant share of infections are very mild or completely without symptoms. Testing everyone to find the huge number of hidden cases cannot possibly work worldwide. As long as there is hidden COVID-19 elsewhere in the world, the benefit of identifying everyone with the illness in a particular area is limited. The disease simply bounces back, as soon as there is a reduction in containment efforts.
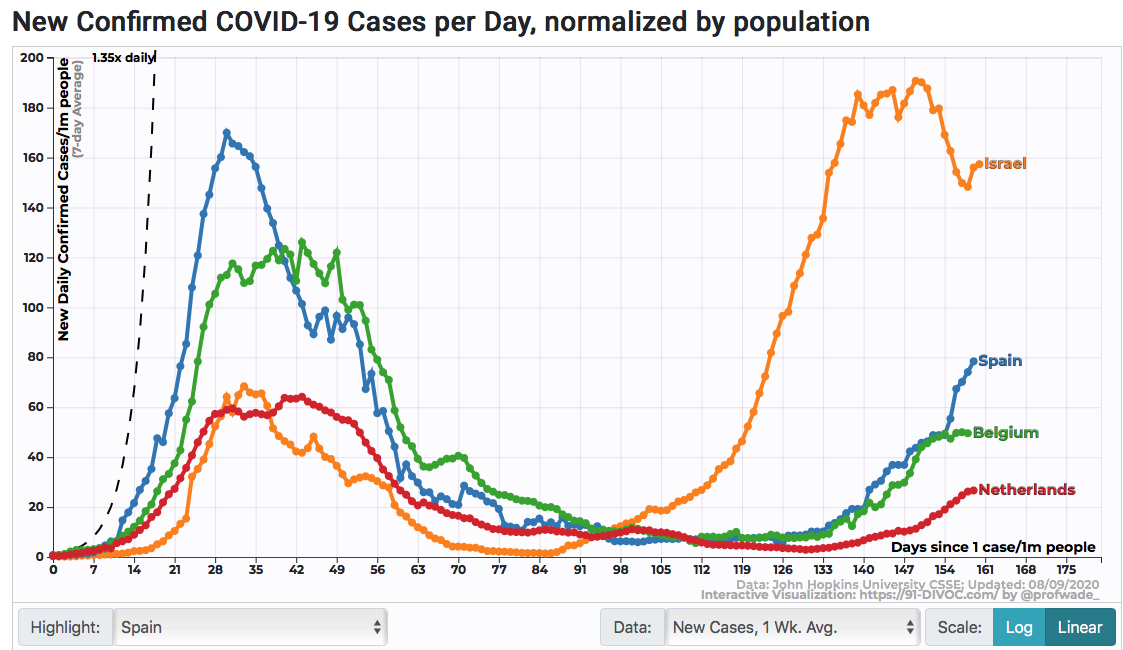
Figure 1. One-week average new confirmed COVID-19 cases in Israel, Spain, Belgium and Netherlands. Chart made using data as of August 8, 2020 using an Interactive Visualization available at https://91-divoc.com/pages/covid-visualization/ based on Johns Hopkins University CSSE database.
We are also discovering that efforts to contain what is essentially a hidden illness are very damaging to the world economy. Shutdowns in particular lead to many unemployed people and riots. Social distancing requirements can make investments unprofitable. Cutting off air flights leads to a huge loss of tourism and leaves farmers with the problem of how to get their fruit and vegetable crops picked without migrant workers. If COVID-19 is very widespread, contact tracing simply becomes an exercise in frustration.
Trying to identify the many asymptomatic carriers of COVID-19 is surprisingly difficult. The cost is far higher than the cost of the testing devices.
At some point, we need to start lowering expectations regarding what can be done. The economy can protect a few members, but not everyone. Instead, emphasis should be on strengthening people’s immune systems. Surprisingly, there seems to be quite a bit that can be done. Higher vitamin D levels seem to be associated with fewer and less severe cases. Better diet, with more fruits and vegetables, is also likely to be helpful from an immunity point of view. Strangely enough, more close social contacts may also be helpful.
In the remainder of this post, I will explain a few pieces of the COVID-19 problem, together with my ideas for modifications to our current strategy.
Recent News About COVID-19 Has Been Disturbingly Bad
It is becoming increasingly clear that COVID-19 is likely to be here for quite some time. The World Health Organization’s director recently warned, “. . . there’s no silver bullet at the moment and there might never be.” A recent Wall Street Journal article is titled, “Early Coronavirus Vaccine Supplies Likely Won’t Be Enough for Everyone at High Risk.” This article relates only to US citizens at high risk. Needless to say, creating enough vaccine for both high and low risk individuals, around the world, is a long way away.
We are also hearing that vaccines may be far less than 100% effective; 50% effective would be considered sufficient at this time. Two doses are likely to be needed; in fact, elderly patients may need three doses. The vaccine may not work for obese individuals. We don’t yet know how long immunity from the vaccines will last; a new round of injections may be needed each year.
A new report confirms that asymptomatic patients with COVID-19 are indeed able to spread the disease to others.
Furthermore, the financial sector is increasingly struggling with the adverse impact shutdowns are having on the economy. If it becomes necessary to completely “write off” the tourism industry, economies around the world will struggle with permanent job loss and debt defaults.
Shutdowns Don’t Work for Businesses and the Financial System
There are many issues involved:
(a) Shutdowns tend to lead to huge job loss. Riots follow, as soon as people have a chance to express their unhappiness with the situation.
(b) If countries stop importing migrant workers, there is likely to be a major loss of fruits and vegetables that farmers have planted. No matter how much money is printed, it does not replace these lost fruits and vegetables.
(c) Manufacturing supply lines don’t work if raw materials and parts are not available when needed. Because of this, a shutdown in one part of the world tends to have a ripple effect around the world.
(d) Social distancing requirements for businesses are problematic because they lead to less efficient use of available space. Businesses can serve fewer customers, so total revenue is likely to fall. Employees may need to be laid off. Fixed costs, such as debt, become more difficult to pay, making defaults more likely.
Shutdowns cause a major problem for the economy, because, with many people out of the workforce, the total amount of finished goods and services produced by the economy falls. Broken supply lines and reduced efficiency tend to make the problem worse. World GDP is the total amount of goods and services produced. Thus, by definition, total world GDP is reduced by shutdowns.
Governments can institute benefit programs for citizens to try to redistribute what goods and services are available, but this will not fix the underlying problem of many fewer goods and services actually being produced. Citizens will find that some shelves in stores are empty, and that many airline seats are unavailable. They will find that some goods are still unaffordable, even with government subsidies.
Governments can try to give loans to businesses to help them through the financial problems caused by new rules, such as social distancing, but it is doubtful this approach will lead to new investment. For example, if social distancing requirements mean that new buildings and vehicles can only be used in an inefficient manner, there will be little incentive for businesses to invest in new buildings and vehicles, even if low-interest loans are available.
Furthermore, even if there might be opportunities for new, more efficient, businesses to be added, the subsidization of old inefficient businesses operating at far below capacity will tend to crowd out these new businesses.
People of Many Ages Soon Become Unhappy with Shutdowns
Young people expect hands-on learning experiences at universities. They also expect to be able to meet possible future marriage partners in social settings. They become increasingly unhappy, as shutdowns drag on.
The elderly need to be protected from COVID-19, but they also need to be able to see their families. Without social interaction, their overall health tends to decline.
We Are Kidding Ourselves If We Think a Vaccine Will Make the Worldwide COVID-19 Problem Disappear
Finding a vaccine that works for 100% of the world’s population seems extremely unlikely. Even if we do find a vaccine or drug treatment that works, being able to extend this solution to poor countries around the world is likely to be a slow process.
If we look back historically, pretty much all of the improvement in the U. S. crude death rate (number of deaths divided by total population) has come from conquering infectious diseases.

Figure 2. Crude mortality rates in the United States in chart from Trends in Infectious Disease Mortality in the United States During the 20th Century, Armstrong et al, JAMA, 1999.
The catch is that since 1960, there hasn’t been an improvement in infectious disease mortality in the United States, according to an article in the Journal of the American Medical Society. As progress has been made on some longstanding diseases such as hepatitis, new infectious diseases such as HIV/AIDS have arisen. Also, the biggest category of infectious disease remaining is “influenza and pneumonia,” and little progress has been made in reducing its death rate in the United States. Figure 3 shows one chart from the article.

Figure 3. Mortality due to influenza or HIV/AIDS, in chart from Infectious Disease Mortality Trends in the United States, 1980-2014 by Hansen et al., JAMA, 2016.
With respect to HIV/AIDS, it took from the early 1980s until 1997 to start to get the mortality rate down through drugs. A suitable vaccine has not yet been created.
Furthermore, even when the US was able to reduce the mortality from HIV/AIDS, this ability did not immediately spread to poor areas of the world, such as Sub-Saharan Africa. In Figure 4, we can see the bulge in Sub-Saharan Africa’s crude death rates (where HIV/AIDS was prevalent), relative to death rates in India, where HIV/AIDS was less of a problem.

Figure 4. Crude death rates for Sub-Saharan Africa, India, the United States, and the World from 1960 through 2018, based on World Bank data.
While the medical system was able to start reducing the mortality of HIV/AIDS in the United States about 1996-1997 (Figure 3, above), a 2016 article says that it was still very prevalent in Sub-Saharan Africa in 2013. Major issues included difficulty patients had in traveling to health care sites and a lack of trained personnel to administer the medication. We can expect these issues to continue if a vaccine is developed for COVID-19, especially if the new vaccine requires more than one injection, every year.
Another example is polio. A vaccine for polio was developed in 1955; the disease was eliminated in the US and other high income countries in about the next 25 years. The disease has still not been eliminated worldwide, however. Poor countries tend to use an oral form of the vaccine that can be easily administered by anyone. The problem with this oral vaccine is that it uses live viruses which themselves can cause outbreaks of polio. Cases not caused by the vaccine are still found in Afghanistan and Pakistan.
These examples suggest that even if a vaccine or fairly effective treatment for COVID-19 is discovered, we are kidding ourselves if we think the treatment will quickly transfer around the world. To transfer around the world, it will need to be extremely inexpensive and easy to administer. Even with these characteristics, the eradication of COVID-19 is likely to take a decade or more, unless the virus somehow disappears on its own.
The fact that COVID-19 transmits easily by people who show no symptoms means that even if COVID-19 is eradicated from the high-income world, it can return from the developing world, unless a large share of people in these advanced countries are immune to the disease. We seem to be far from that situation now. Perhaps this will change in a few years, but we cannot count on widespread immunity any time soon.
Containment Efforts for a Disease with Many Hidden Carriers Is Likely to Be Vastly More Expensive than One in Which Infected People Are Easily Identifiable
It is easy to misunderstand how expensive finding the many asymptomatic carriers of a disease is. The cost is far higher than the cost of the tests themselves, because the situation is quite different. If people have serious symptoms, they will want to stay home. They will want to give out the names of others, if they can see that doing so might prevent someone else from catching a serious illness.
We have the opposite situation, if we are trying to find people without symptoms, who might infect others. We need to:
- Identify all of these people who feel well but might infect others.
- Persuade these people who feel well to stay away from work or other activities.
- Somehow compensate these people for lost wages and perhaps extra living expenses, while they are in quarantine.
- Pay for all of the tests to find these individuals.
- Convince these well individuals to name those whom they have had contact with (often their friends), so that they can be tested and perhaps quarantined as well.
Perhaps a few draconian governments, such as China, can handle these problems by fiat, and not really compensate workers for being unable to work. In other countries, all of these costs are likely to be a problem. Because of inadequate compensation, exclusion from work is not likely to be well received. Quarantined people will not want to report which friends they have seen recently, if the friends are likely also to lose wages. In poor countries, the loss of income may mean the loss of the ability to feed a person’s family.
Another issue is that “quick tests” are likely to be used for contact tracing, since “PCR tests,” which tend to be more accurate, often require a week or more for laboratory processing. Unfortunately, quick tests for COVID-19 are not very accurate. (Also a CNN report.) If there are a lot of “false positives,” many people may be needlessly taken out of work. If there are a lot of “false negatives,” all of this testing will still miss a lot of carriers of COVID-19.
A Major Benefit of Rising Energy Consumption Seems to Be Better Control Over Infectious Diseases and a Falling Crude Death Rate
I often write about how the world’s self-organizing economy works. The growth in the world’s energy consumption since the advent of fossil fuels has been extremely important.
Figure 5. World Energy Consumption by Source, based on Vaclav Smil estimates from Energy Transitions: History, Requirements and Prospects, together with BP Statistical Data on 1965 and subsequent
The growth in world energy consumption coincided with a virtual explosion in human population.

One of the ways that fossil fuel energy is helpful for population growth is through drugs to fight epidemics. Another way is by making modern sanitation easy. A third way is by ramping up food supplies, so that more people can be fed.
Economic shutdowns lead to reduced energy consumption, partly because energy prices tend to fall too low for producers. They cut back on production because of unprofitability.
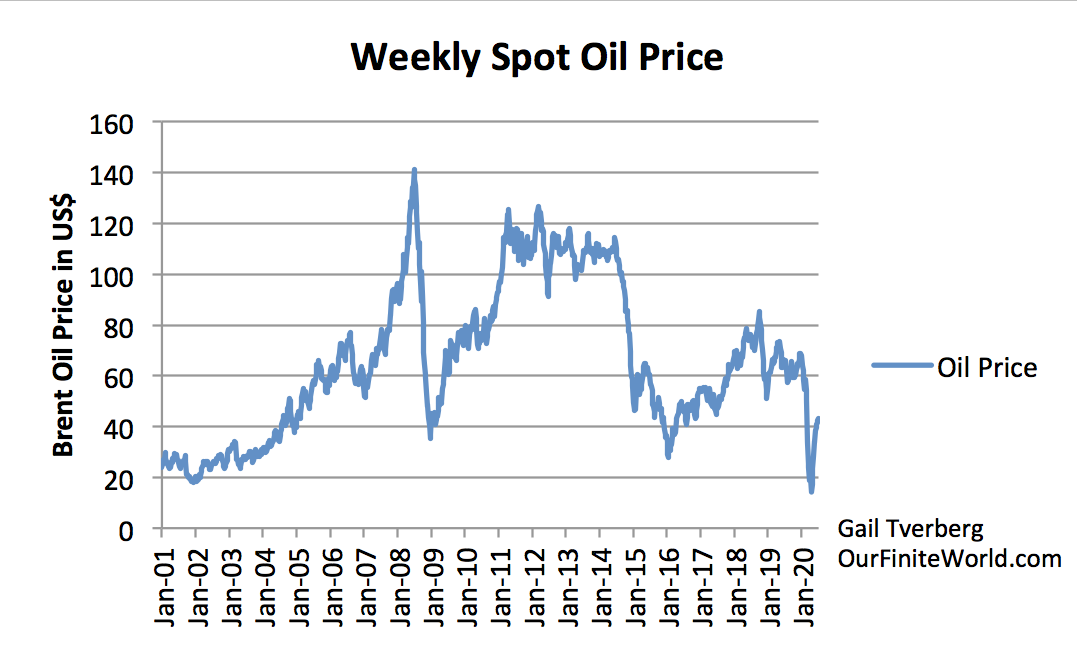
Figure 7. Weekly average spot oil prices for Brent, based on data of the US Energy Information Administration.
Given this connection between energy supply and population, we should not be surprised if shutdowns tend to lead to an overall falling world population, even if COVID-19 by itself is expected to have a small mortality rate (perhaps 1% of those infected). Poor countries, especially, will find that laid off workers cannot afford adequate food supplies. This makes poor members of those economies more susceptible to diseases of many kinds and to starvation.
Epidemiologists Based Their Models on Diseases Which Are Easily Identifiable and Have High Mortality Rates
It is clear that an easily identifiable illness with a high mortality rate can be easily contained. A difficult-to-identify disease, which has a very low mortality rate for many segments of the population, is very different. Members of segments of the population who usually get only a light case of the disease are likely to become more and more unhappy as containment efforts drag on. Models based on very different types of pandemics are likely to be misleading.
We Need to Somehow Change Course
The message that has been disseminated has been, “With containment efforts plus vaccine, we can stop this disease.” In fact, this is unlikely for the foreseeable future. Continuing in the same direction that has not been working is a lot like banging one’s head against a wall. It cannot be expected to work.
Somehow, expectations need to be lowered regarding what containment efforts can do. The economy can perhaps protect a few high-risk people, but it cannot protect everyone. Unless COVID-19 stops by itself, a significant share of the world’s population can be expect to catch COVID-19. In fact, some people may get the disease multiple times over their lifetimes.
If we are forced to live with some level of COVID-19 (just as we are forced to live with some level of forest fires), we need to make this situation as painless as possible. For example,
- We need to find ways to make COVID-19 as asymptomatic as possible by easy changes to diet and lifestyle.
- We also need to find inexpensive treatments, especially ones that can be used outside of a hospital setting.
- We need to keep the world economy operating as best as possible, if we want to stay away from a world population crash for as long as possible.
We cannot continue to post articles which seem to say that a spike in COVID-19 cases is necessarily “bad.” It is simply the way the situation has to be, if we don’t really have an effective way of containing the coronavirus. The fact that young adults build up immunity, at least for a while, needs to be viewed as a plus.
Some Ideas Regarding Looking at the Situation Differently
(1) The Vitamin D Issue
There has been little publicity about the fact that people with higher vitamin D levels seem to have lighter cases of COVID-19. In fact, whole nations with higher vitamin D levels seem to have lower levels of deaths. Vitamin D strengthens the immune system. Sunlight raises vitamin D levels; fish liver oils and the flesh of fatty fishes also raise vitamin D levels.
Figure 8 shows cumulative deaths per million in a few low and high vitamin D level areas. The death rates are strikingly lower in the high vitamin D level countries.
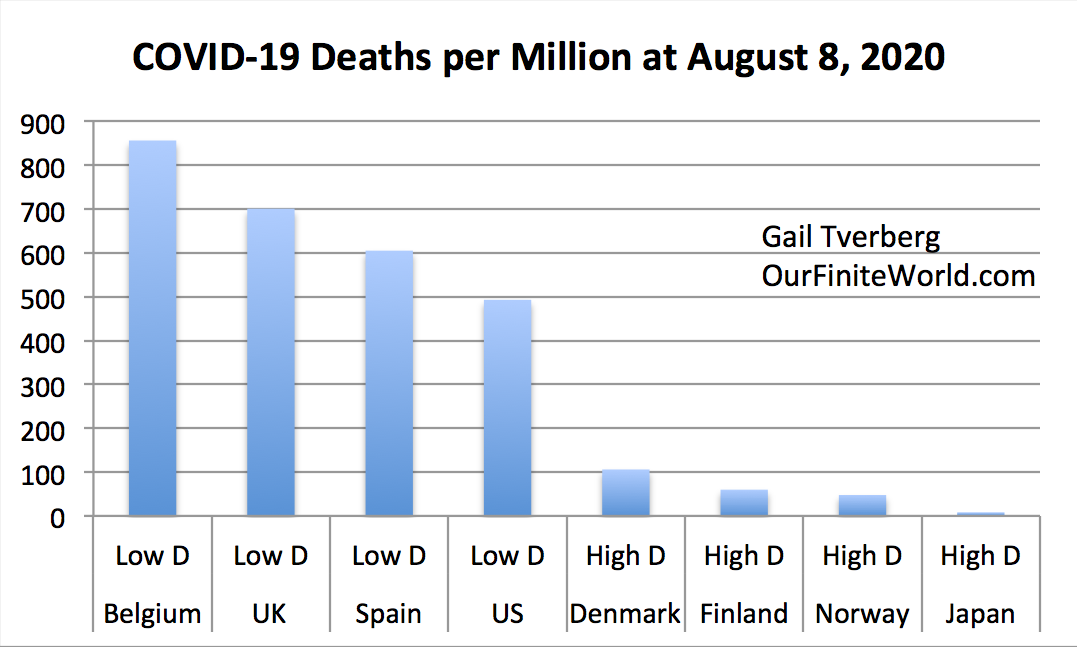
Figure 8. COVID-19 deaths per million as of August 8, 2020 for selected countries, based on data from Johns Hopkins CSSE database.
The vitamin D issue may explain why dark skinned people (such as those from Southeast Asia and Africa) tend to get more severe cases of COVID-19 when they move to a low sunlight area such as the UK. Skin color is an adaptation to different levels of the sun’s rays in different parts of the world. People with darker skin color have more melatonin in their skin. This makes the production of vitamin D less efficient, since equatorial regions receive more sunlight. The larger amount of melatonin works well when dark-skinned people live in equatorial regions, but less well away from the equator. Vitamin D supplements might mitigate this difference.
It should be noted that the benefit of sunlight and vitamin D in protecting the immune system has long been known, especially with respect to flu-like diseases. In fact, the use of sunlight seems to have been helpful in mitigating the effects of the Spanish Flu outbreak in 1918-1919, over 100 years ago!
One concern might be whether increased sunlight raises the risk of melanoma, a deadly form of skin cancer. I have not researched this extensively, but a 2016 study indicates that that sensible sun exposure, without getting sunburn, may decrease a person’s risk of melanoma, as well as provide protection against many other types of diseases. Non-melanoma skin cancers may increase, but the mortality risk of these skin cancers is very low. On balance, the study concludes that the public should be advised to work on getting blood levels of at least 30 ng/ml.
(2) Other Issues
Clearly, better health in general is helpful. Eating a diet with lot of fruits and vegetables is helpful, as is getting plenty of exercise and sunshine. Losing weight will be helpful for many.
Having social contact with other people tends to be helpful for longevity in general. In fact, several studies indicate that church-goers tend to have better longevity than others. Churchgoers and those with many social contacts would seem to have more contact with microbes than others.
A recent article says, Common colds train the immune system to recognize COVID-19. Social distancing tends to eliminate common colds as well as COVID-19. Quite possibly social distancing is counterproductive, in terms of disease severity. Epidemiologists have likely never considered this issue, since they tend to consider only very brief social distancing requirements.
A person wonders how well the immune systems of elderly people who have been cut off from sharing microbes with others for months will work. Will these people now die when exposed to even very minor illnesses? Perhaps a slow transition is needed to bring families back into closer contact with their loved ones.
People’s immune systems can protect them from small influxes of viruses causing COVID-19, but not from large influxes of these viruses. Masks tend to protect against large influxes of the virus, and thus protect the wearer to a surprising extent. Models suggest that clear face shields also provide a considerable amount of this benefit. People with a high risk of very severe illness may want to wear both of these devices in settings they consider risky. Such a combination might protect them fairly well, even if others are not wearing masks.
Conclusions – What We Really Should Be Doing
Back at the time we first became aware of COVID-19, following the recommendations of epidemiologists probably made sense. Now that more information is unfolding, our approach to COVID-19 needs to change.
I have already laid out many of the things I think need to be done. One area that has been severely overlooked is raising vitamin D levels. This is being discussed in the medical literature, but it doesn’t seem to get into the popular press. Even though the connection is not 100% proven, and there are many details to be worked out, it would seem like people should start raising their vitamin D levels. There seems to be little problem with overdosing on vitamin D, except that sunburns are not good. Until we know more, a level of 30 ng/ml (equivalent to 75 nmol/L) might be a reasonable level to aim for. This is a little above the mean vitamin D level of Norway, Finland, and Denmark.
Social distancing requirements probably need to be phased out. A concern might be temporarily excessive patient loads for hospitals. Large group meetings may need to be limited for a time, until this problem can be overcome.
No comments:
Post a Comment